
Saving health systems money, improving patient outcomes and provider satisfaction

Saving health systems money, improving patient outcomes and provider satisfaction
How We Got Started Setting Up Clinically Integrated Networks
In 2012 our sponsoring hospital system set up a Clinically Integrated Network. The “change agents” were the physician leaders. We, the physicians, wanted to prepare for whatever change was coming, and we knew it would involve some “Fee-for-Value” approach with a population health approach.
Clinically Integrated Networks that are hospital or system sponsored almost always focus on the healthcare spend of the sponsoring organization. This approach provides operation and financial safety for the physicians and the leadership of the Clinically Integrated Network to hone their craft, identify and engage high cost and soon to be high cost patients which drive the majority of the spend, and control their costs and improve the quality of care these folks receive.
There are almost no CINs that continuously save money and distribute to their member providers year after year. Our approach targets the high cost patients, and by identifying them and engaging the primary care providers, we saved money immediately and provided a distribution to the participating physicians in every year of our operation. The Quality Metrics improved every year as well.
The Christ Hospital Employee Health Plan Medical Costs Under Clinically Integrated Network
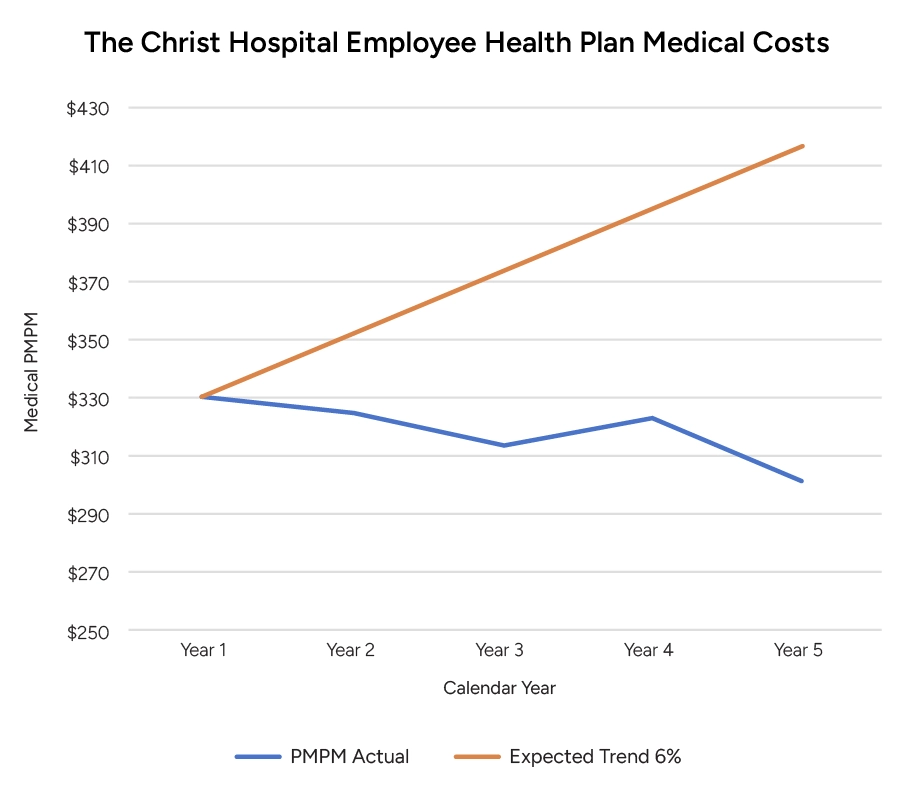
We based our projection on a Per Member Per Month actuarial analysis, which would be agreeable to all the stakeholders. The Hospital System and its leadership, the actuaries, and compliance; including third party auditors who certifies the savings.
Let us show you how to do it. You have the data systems in place. The physicians and other advanced practice providers will be bound to the system like never before. The financial well-being of your system will be improved within the first year or two of operation.